Virtual Clinic Visit: Peripheral Vascular Case Study
Introduction
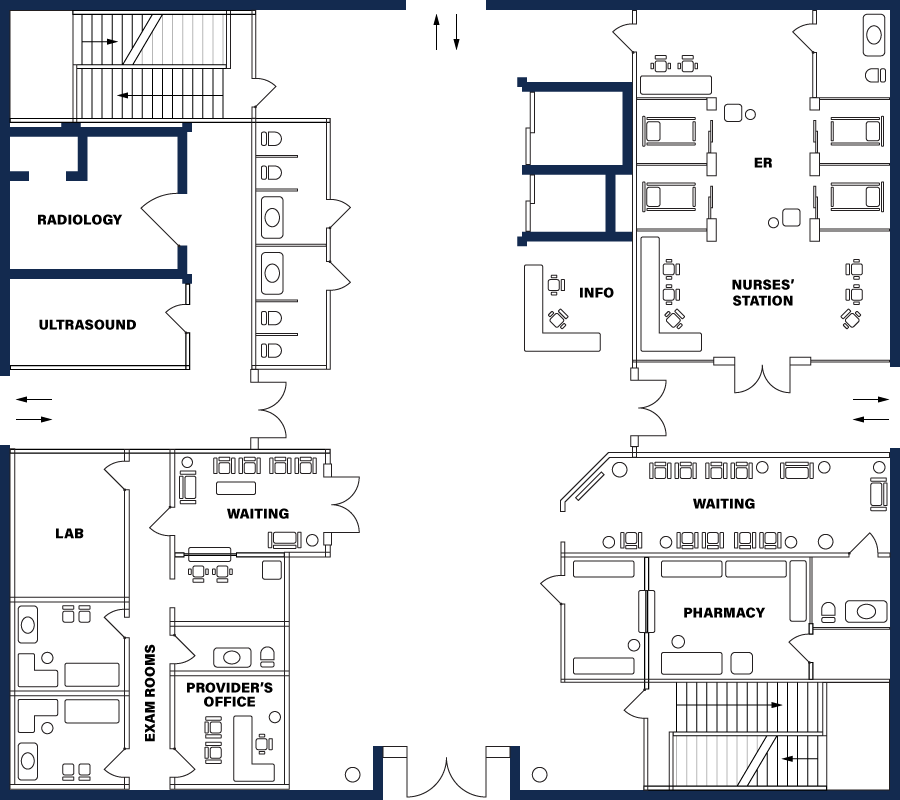
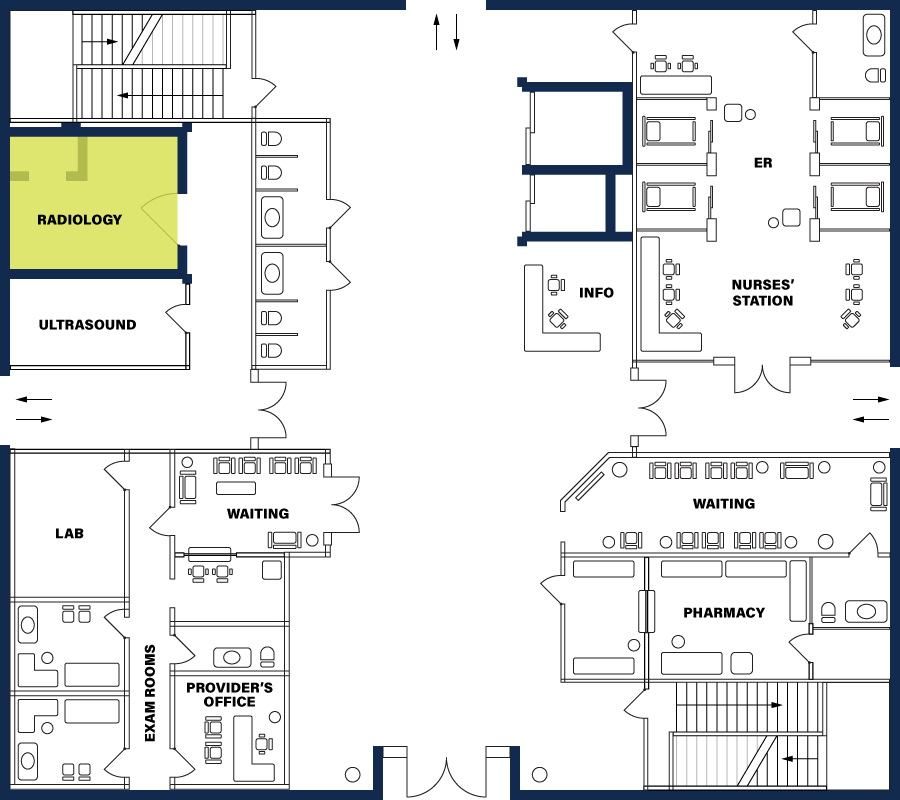
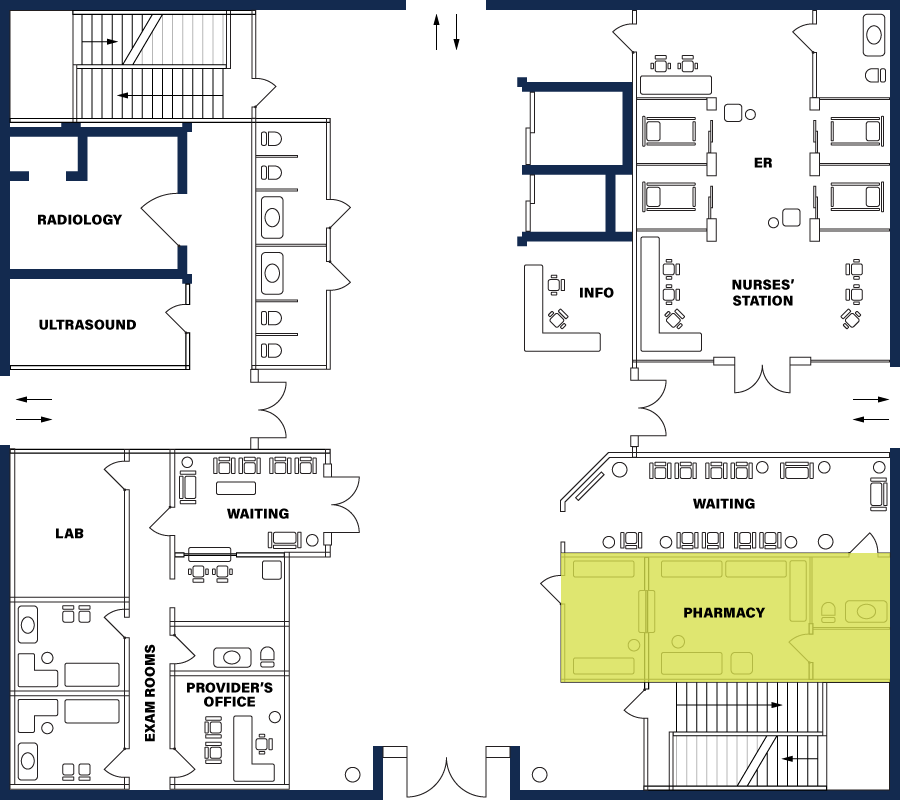
Welcome to the Virtual Clinic! You will be visiting various rooms in the clinic collecting information and participating in activities that will lead you to a final summary. For each room that is available to visit, please make sure you complete the activity and use the information to make decisions for your patient. Please select the first available room you would like to visit from the Directory.



Nurse’s Station


Review Records
Full Name:
Pamela Penn
Gender:
Woman
Age:
52 years old
Address
181 Berkeley Ridge Dr. Lubbock, TX 29229
Height:
5’6"
Weight:
225 lbs. (BMI= 36.3 [obese])
Vital Signs:
Blood Pressure (BP): 132/90
Oxygen Saturation (O2): 100%
Pulse Rate (PR): 92
Respiratory Rate (RR): 18
Temperature: 98 degrees Fahrenheit
Personal History (PH)
Married for 30 years; 2 children (son 23 and daughter 25)
Family History:
Mother: 79, alive and well. Father: 54, deceased, heart attack. No siblings. There is a positive family history of hypertension, CAD, but no history of diabetes or cancers.
Social History:
Alcohol use: 1 or 2 beers each weekend; 5 glasses of wine once a week with dinner
Tobacco use: None
Medical History:
28 years old: Dx with hypertension and began taking an unknown betablocker. Stopped after 6 months because of drowsiness.
20 years old: Dx with peptic ulcer disease, which resolved after three months on cimetidine.
She always uses generic names; describes no history of cancer, lung disease, or previous heart disease.
Surgical History
Bunionectomy (28 years old); total abdominal hysterectomy (TAH) with bilateral salpingo-oophorectomy (BSO) 10 years ago.
Allergies:
Penicillin; experienced rash and hives in 1985
Immunization History:
Tdap (last received 15 years ago); Up to date with covid and flu vaccinations.
Medications Currently Taking:
HCTZ 12.5 mg; OTC Ibuprofen (Advil); multivitamin
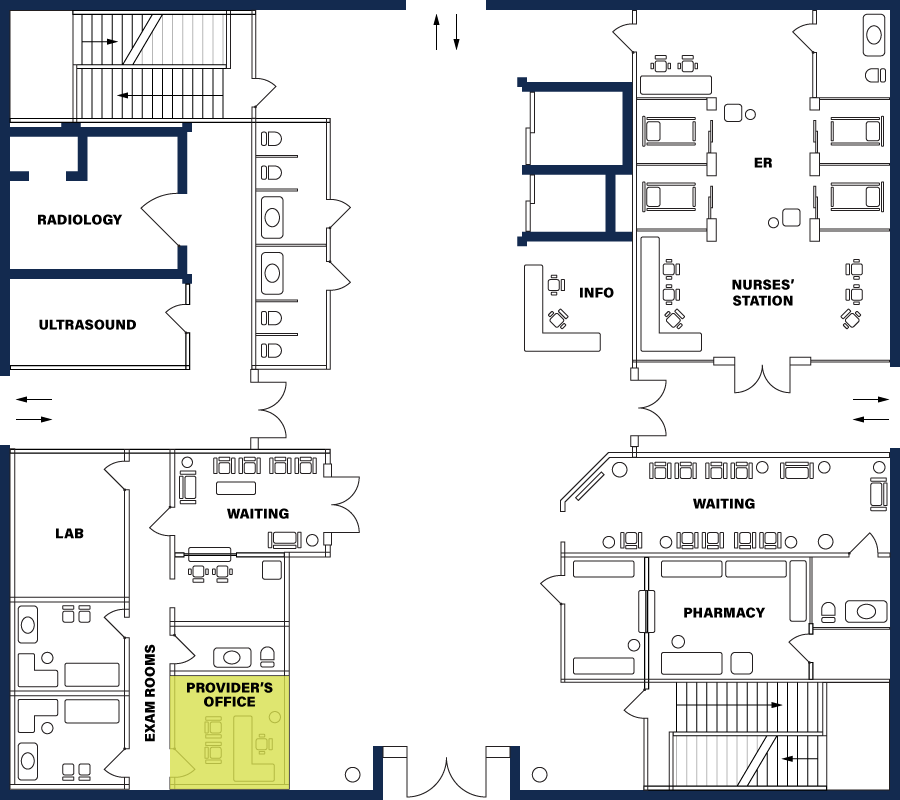
The Provider’s Office
Today, you see Pamela Penn, who is new to you, but an established patient at the clinic.

Feedback
The patient is complaining of chest discomfort, which is the chief complaint. She also mentioned her feet swell at the end of the day and she is obese which you should be aware of and include in your medical note and decision making, but they are not the chief complaint.
Feedback
- Onset (Correct, 1-2 weeks)
- Location (Correct, left side of chest and arm)
- Duration (Correct, few seconds to 1 minute, resolve quickly with rest)
- Characteristic (Correct, dull ache)
- Aggravating factors (Correct, worsened when walking dog, gardening, walking)
- Relieving factors (Correct, relieved by rest, has tried ibuprofen as well)
- Timing (Correct, occurs with resolves quickly
- Severity (correct, 5/10 discomfort)
Feedback
Chest pain that occurs with activity and resolves quickly with rest is called stable angina. It is a symptom of coronary artery disease. Acute coronary syndrome is an acute cardiac event that would not present intermittently over weeks. Heart failure is high on the differential given her pain and the swelling in her feet. Costochondritis would present with different history and would be reproducible on examination. GERD is another consideration, it can also worsen with activity, but it would typically have heartburn symptoms, and symptoms when lying down.
The Exam Room
Questions
Feedback
The NP should do a thorough cardiovascular examination. A peripheral vascular, and respiratory examination will be important to assess as well.
Exam Results:
General exam: obese ; CV: murmur or extra heart sound appreciated.
Heart rate is 96 on exam so it is difficult to distinguish the extra sound.
1+ pitting edema to bilateral lower extremities (BLE). Remainder of the exam is normal.
